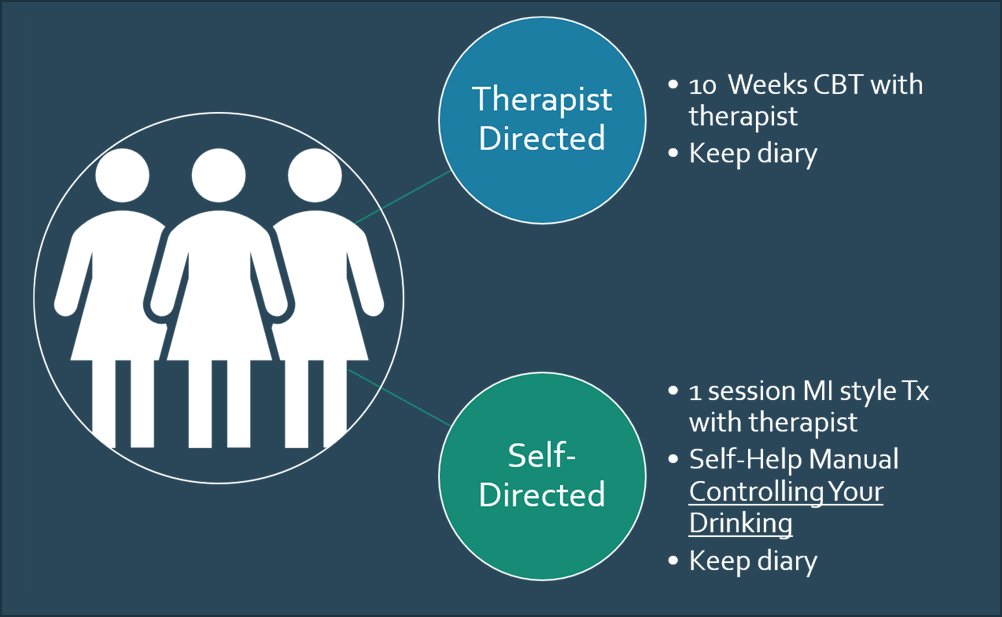
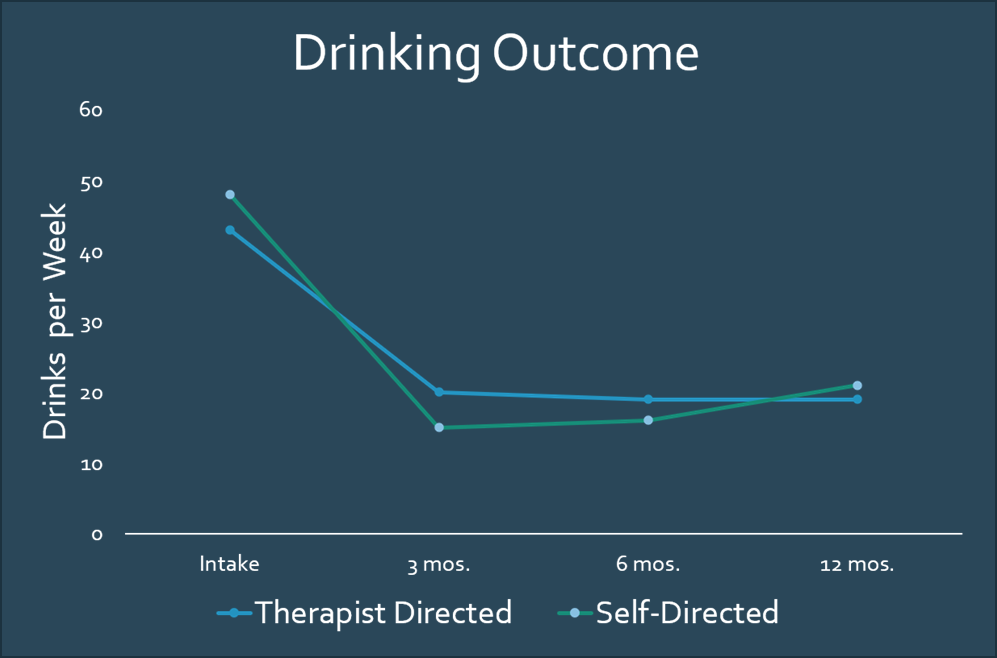
| The Motivational Interviewing approach is an evidence-based practice; it has been methodically studied, replicated, and proven effective. Its discovery, on the other hand, was by accident. One of the founders, Bill Miller, a young psychologist in training, was assigned to serve those with the second most common diagnosis in his work facility: alcoholism. The popular model of treatment, at that time, presumed those living with alcoholism to be in denial, resistant to change, and manipulative. The prescribed treatment approach: confrontation. Bill chose a different approach. Instead, relying on Rogerian therapy's tenets, Bill presumed his clients to have inherent value, be worthy of respect, and possess the wisdom and capability to make positive changes. He demonstrated unconditional positive regard when working alongside them, listened empathetically, and rolled with their resistance rather than opposing it. From them, he evoked their concerns, motivations, and their own arguments for change. Lo and behold, it worked! Bill researched the approach via several studies for his doctoral dissertation to determine why it worked. What was the special sauce, if any? The design and findings of some of those studies are described below. STUDY 1 Study Design Problem drinkers were assigned to two groups. Therapists gave Group One 10 weeks of Cognitive Behavioral Therapy (CBT) and asked them to keep a diary. Therapists gave Group Two one session of MI-style therapy and a self-help manual, Controlling Your Drinking. The effectiveness of each methodology was measured by how many drinks the clients consumed following treatment. (See illustration below.) Study Outcome The outcome is not what one would predict. As you can see, both the therapist-directed and the self-help group started out drinking between 40 and 50 drinks per week. By month three, both groups had reduced their drinking from 20 to 10 drinks per week, with the self-help group faring slightly better. When asked what helped them, the self-help group members indicated the diary. The brief therapy was as good, if not better, than the more prolonged therapy. Why? Was it because the people who came to the group had already decided to change? Or was it because they chose to keep up with the diary? To answer those questions, Bill and his team set out to replicate the study.
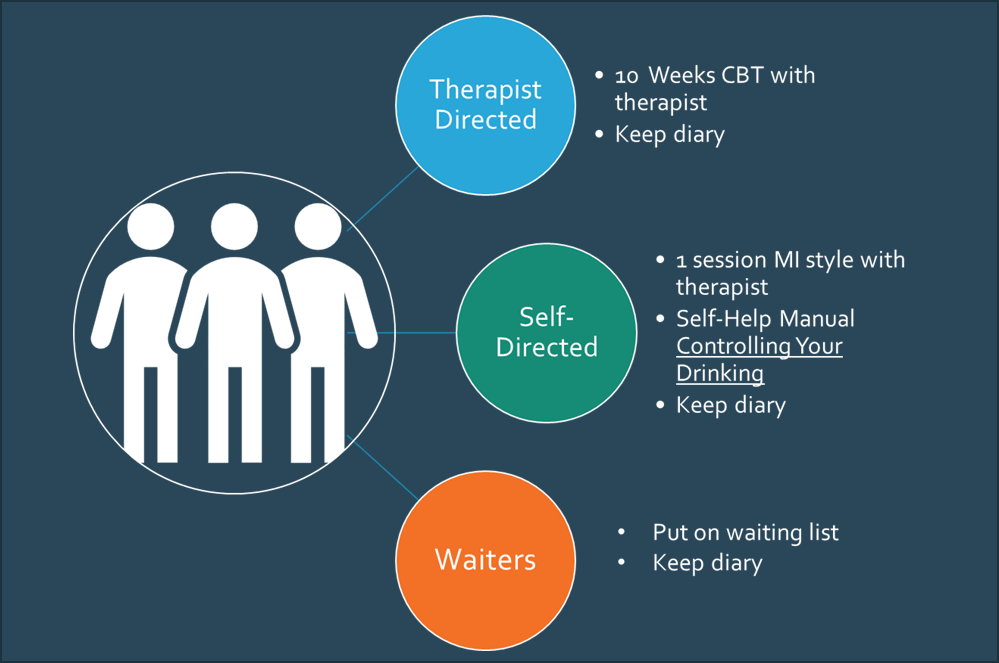
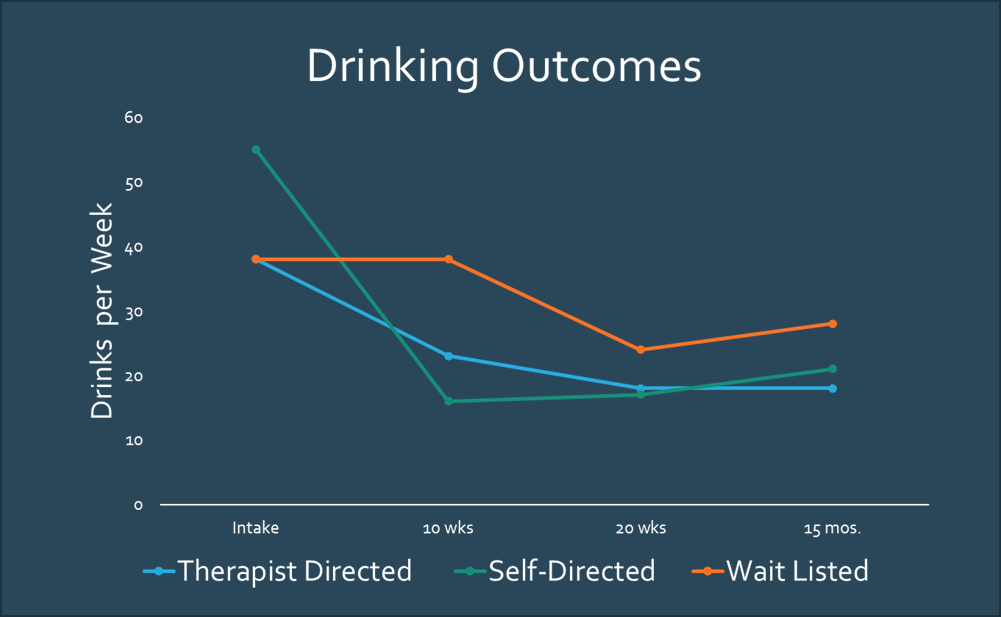
STUDY 2 Study Design Problem drinkers were randomly assigned to three groups. Group One received 10 weeks of Cognitive Behavioral Therapy and kept a diary. Group Two received one session of Motivational Interviewing style therapy, the self-help manual, Controlling Your Drinking, plus a diary. Group 3 was put on a waiting list, asked to keep a diary, and informed that somebody would contact them in 10 weeks. Study Outcome Again, the self-help group started worse and ended up better. And, the waiters? Well, they waited. The implied message of being put on a waiting list was this: you're not expected to get better until we provide you with treatment.
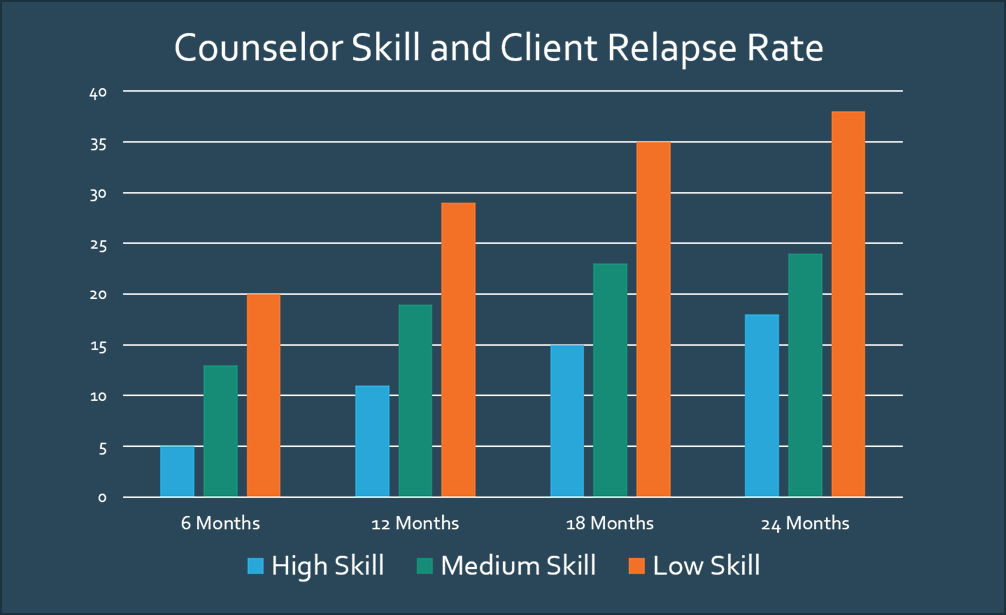
Important Sidebar: What is the meaning of this finding for VR programs with Order of Selection waiting lists? Is it unintentionally implying that clients can't improve their lot or seek work until VR assists? Let's note that this same study revealed that when given only one session of therapy, a self-help resource, and an expectation of improvement, people didn't wait! In fact, they outperformed those with more resources! How can we apply this finding to VR agencies with waiting lists today? One suggestion is for the VR professional to set a "Don't wait for VR to get started" expectation, and provide rich resources and referral information to support their start. Also, it suggests that it would be worthwhile to make the required 6-month contacts of those on waiting lists more meaningful by reaffirming the expectation that people can go ahead and get started, asking questions about their progress to date, and providing brief guidance and compatible resource information to help them along. STUDY 3 Dozens of controlled trials revealed the effectiveness of brief interventions, but not all counselors using the same skill set had the same outcomes. What was the special sauce of those who were successful? In the study illustrated below, Dr. Miller and his colleagues observed counselors employing the same set of skills and noted that some counselors used accurate empathy. Those who evidenced more genuine empathy had an inverse relationship with relapse rates; the more accurate empathy they employed, the fewer relapses clients had. The technique would fall flat if it were employed without authenticity and the expression of accurate empathy. Well, there it was, the special sauce: empathy.
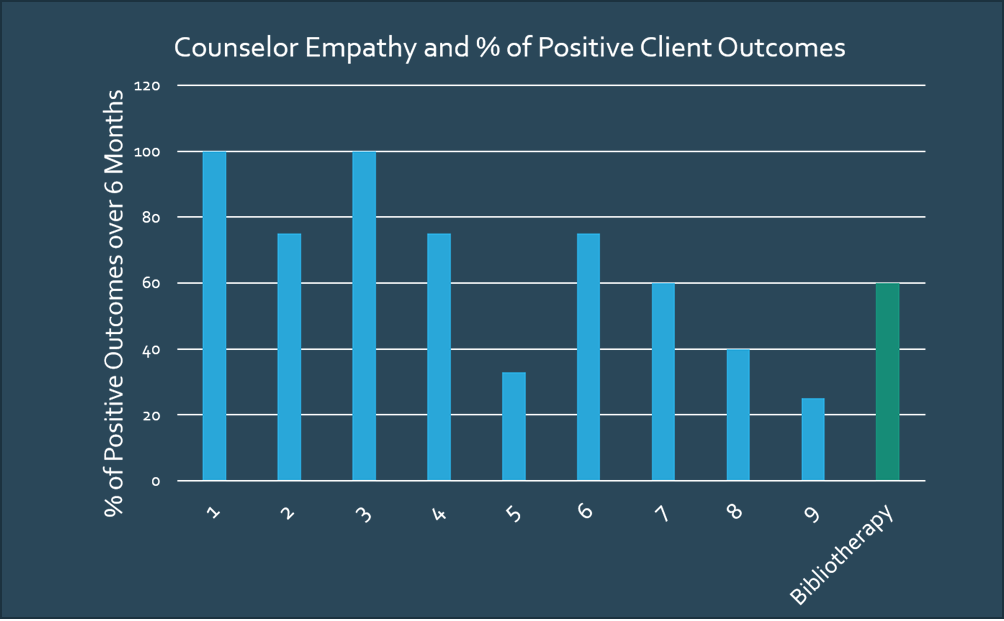
STUDY 4 To confirm their findings, Dr. Miller and his team conducted another study. When measured for "accurate empathy," the five counselors who demonstrated the most empathy outperformed the self-help group.
Summary As the studies above demonstrate, Motivational Interviewing works. In the next modules, we learn about the underlying principles (spirit) of MI and the foundational skills of MI. |